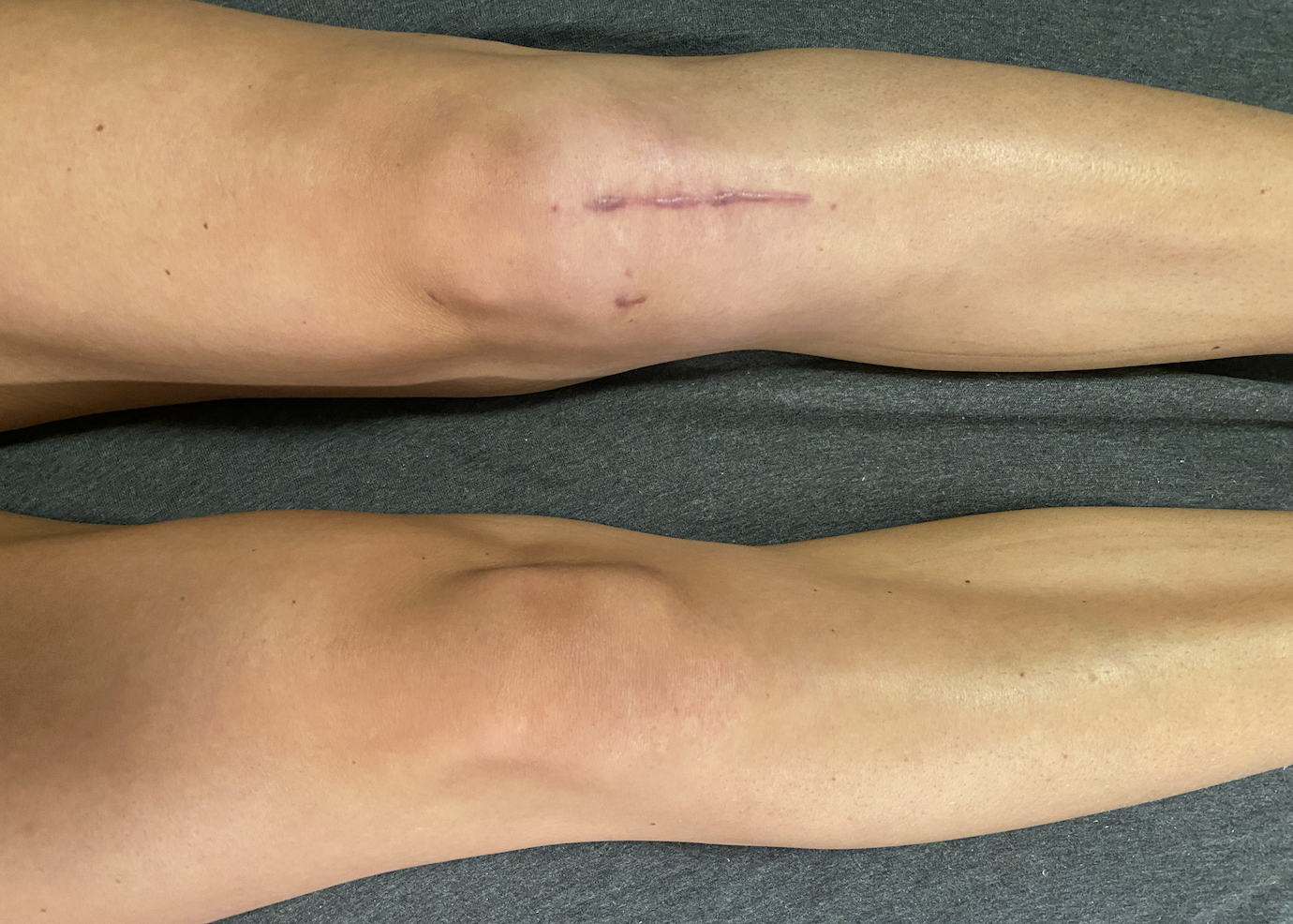
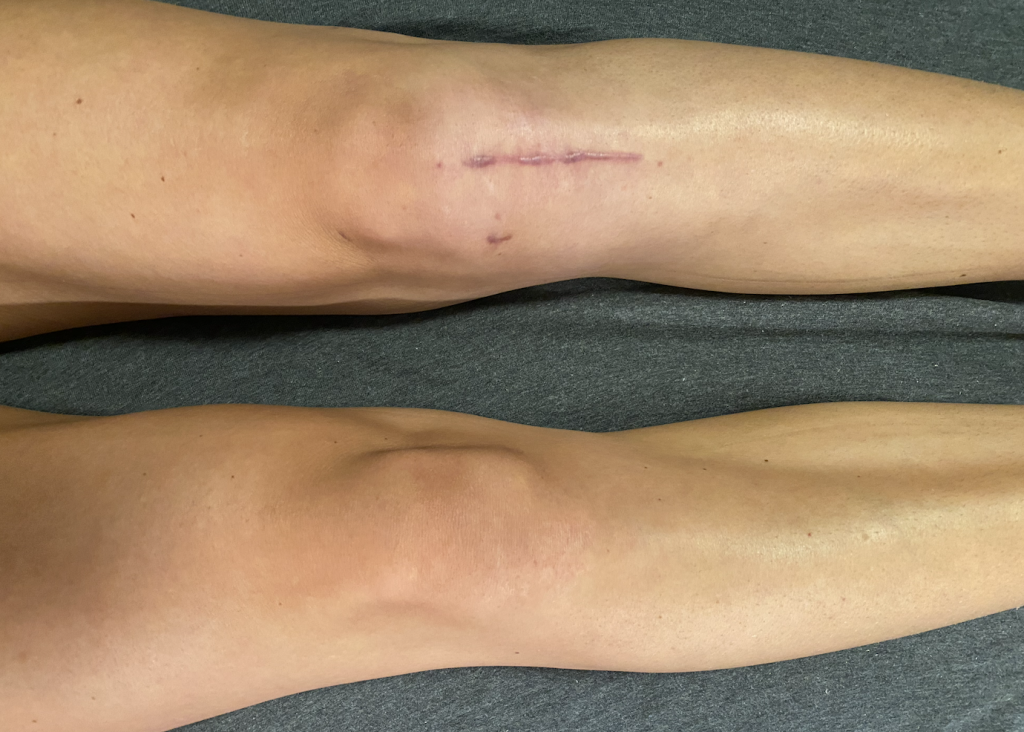
Where did your quad muscle go?!
To work on getting back your quad muscles, prioritize:
- Using neuromuscular electrical stimulation (from your physiotherapsit)
- Active quadriceps squeezes
- Range of motion exercises
- External cues like a metronome
Look, I’ve been there – you got injured, you did the pre-operative rehabilitation, and now post-op you look at your legs and one of them has NO muscle!
Firstly, know that you are not alone and this is completely normal for post-operative knee surgeries, especially ACLR (anterior cruciate ligament reconstruction). We go through something called Arthrogenic Muscle Inhibition (AMI) – where our nervous system and brain change the firing of our neurons to our muscles, our quadriceps muscles in the case of traumatic knee injuries.
As a patient, this is experienced as muscle size loss, lack of ability to activate or squeeze the muscle voluntarily, and reduced muscle strength.
This tends to happen since our knee joint has undergone a traumatic event and our nervous system as a result is receiving and relaying information related to increased pain and swelling, a change in sensory information, and damage to receptors in the knee itself. More research still needs to be done in this area because, as always, our bodies are complex, but at the moment this is the generally accepeted understanding of why this phenomenon may occur.
How do you counter this post-operatively or after your ACL injury?
Current ACLR Post-Operative Guidelines from Aspetar recommend:
- The use of NMES, neuromuscular electrical stimulation, to help with the recruit of the motor units of the quad muscles in early stage rehab
- I’d recommend having your physio show you how to use a muscle stim machine, but they are readily available for public use and are a great piece of equipment for the early rehab phases
The University of Delaware Physical Therapy has been researching this area and recommends:
- Session-by-session NMES dosage and programming according to 50% of the patient’s max voluntary contraction for the muscle stim unit settings
- Using these settings for 10-15 minutes in each session where the patient is NOT doing an additional voluntary contraction as the muscle stim is on
- They go into education to the patient around discomfort of the intensity of these settings – mostly because it IS uncomfortable (but safe), and it requires that level of intensity to reap the benefits
- They recommend using large pads to help reduce some of this discomfort
- The paper they wrote outlining the standards clinicians should be using is here. E3Rehab does a great Q&A podcast that interviews the authors which you can listen to here.
Exercise Rehabilitation
To continue working on direct quad muscle use, Aspetar also recommends early exercise rehabilitation (this should always be guided by your surgery and physiotherapist):
- Active knee range of motion – such as heel slides and quad squeezes
- Early weightbearing (depending on your surgery and restrictions) – walking retraining exercises with crutches and slowly wean off crutches
- Open kinetic chain exercises after the 4th week post-operatively – this should be guided by your physio early on but isometrics can be started and ca slowly progress through range of motion and eventually to weighted knee extensions
- Eccentric quad exercises between 20-60 degrees of knee flexion after 3 weeks post-op – guided by your physiotherapist, you can use a metronome to help overcome the inhibition with external cueing
Use External Cues for Quads – Brain Connection
To address the input and output messages from the muscle <-> brain and spinal cord, we can continue to use different strategies such as external cueing and metronome training.
- Use a metronome for your early squat patterning – 3s down phase, and 2s up phase – this can be partial squats in the early phases of rehab
- Use holds – with a metronome, hold the top squeeze phase of quad extensions for 3-5s
- Eccentric quad extensions – use a metronome to time the lowering phase for 3-5s
Essentially, we are trying to retrain the brain, the motor units in the muscles and the firing of the neurons to get the quad to activate and be able build back strength and size. This is extremely important in the beginning phases of rehab so that your body uses this muscle during the more complex phases of rehab later on and doesn’t create compensations or new ways of NOT using the injured leg. Check with your physio on using NMES and quad specific exercises during your rehab!
If you’ve just injured your ACL, I recommend starting with the ACL Injuries ebook.
References:
- Arhos, Elanna K., et al. “Who’s Afraid of Electrical Stimulation? Let’s Revisit the Application of NMES at the Knee.” journal of orthopaedic & sports physical therapy 54.2 (2024): 101-106.
- Norte G, Rush J, Sherman D. Arthrogenic muscle inhibition: best evidence, mechanisms, and theory for treating the unseen in clinical rehabilitation. Journal of sport rehabilitation. 2021 Dec 9;31(6):717-35.
- Kotsifaki R, Korakakis V, King E, Barbosa O, Maree D, Pantouveris M, Bjerregaard A, Luomajoki J, Wilhelmsen J, Whiteley R. Aspetar clinical practice guideline on rehabilitation after anterior cruciate ligament reconstruction. British journal of sports medicine. 2023 May 1;57(9):500-14.
- Culvenor AG, Girdwood MA, Juhl CB, Patterson BE, Haberfield MJ, Holm PM, Bricca A, Whittaker JL, Roos EM, Crossley KM. Rehabilitation after anterior cruciate ligament and meniscal injuries: a best-evidence synthesis of systematic reviews for the OPTIKNEE consensus. British journal of sports medicine. 2022 Dec 1;56(24):1445-53.
- Gómez-Feria J, Martín-Rodríguez JF, Mir P. Corticospinal adaptations following resistance training and its relationship with strength: a systematic review and multivariate meta-analysis. Neuroscience & Biobehavioral Reviews. 2023 Jun 21:105289.
Article updated Sep 7 2024


